This is a summary of the main evidence used to convict Lucy Letby, with links to many other documents relating to the case and more in-depth articles examining the severe shortcomings in the scientific evidence which led to the conviction. Much of the material comes from the website https://rexvlucyletby2023.com/ of the organisation Science on Trial https://www.scienceontrial.com/. The material in https://rexvlucyletby2023.com/ (now offline, but preserved at https://web.archive.org/web/20230824112701/http://rexvlucyletby2023.com/) was presented to the defence team during the trial but was not used due to rules which prevent the introduction of new expert evidence once a UK criminal trial is underway.
This summary was written by Tom Gibb and Kate Nickalls and reproduced here with their permission (some minor corrections made by Richard Gill).
Lucy Letby (LL) was convicted and sentenced to spend the rest of her life in prison for murdering seven babies and attempting to murder six others between June 2015 and May 2016. The summary of evidence below is organised in rough chronological order to also explain how the investigation against her was conducted. It is accompanied by commentary to explain why both the investigation and evidence collected were flawed:
1) The Statistical Evidence.
In 2016, consultants at the Countess of Chester Hospital (CoCH) became suspicious that LL always appeared to be on duty when babies collapsed or died. These suspicions were later summarised into a data chart of nurses’ shifts produced by the police which, the jury was told, showed that LL was the only nurse present at all 8 deaths (one murder charge was dropped by the court prior to the trial), and 17 incidents of sudden collapses on the unit which were listed in the chart. This gave the very misleading impression to the jury of a correlation that was too much to be coincidence. In fact, there were many more deaths which should have been included in the chart; and most likely very many collapses too.
- The 25 incidents in the Police chart only represented those included in the investigation. Hospital records (obtained by a freedom of information request) show that there were an additional 9 neonatal deaths during this period, for which LL was not charged and when she was not on duty. So, the police table showed only a partial subset of data representing less than half the deaths on the unit. During the trial, no proof was given at all that Lucy had done anything wrong or was in any way the cause of those 25 events.
- The statistical evidence about the 16 non-fatal collapses is even more misleading. The collapses were selected by the hospital consultants because they deemed them suspicious. They did this retrospectively after they had agreed LL herself was suspicious, and the list was restricted to incidents occurring during Lucy’s shifts making it statistically meaningless. The shift data chart does not show any non-fatal incidents/collapses which occurred when Lucy was not on shift. In fact, nobody can say how many such incidents occurred because neither the hospital nor NHS systematically registers incidents/collapses requiring quick action by nurses or doctors.
- Statistics weren’t explicitly used by prosecution, because no detailed statistical analysis was ever carried out; instead they insinuated a statistical correlation via the shift data chart.
- The lack of any formal statistical analysis made it impossible to conclude whether LL’s presence could have been the result of chance. A number of factors would point to a coincidental relation. While other staff indicated on the data chart worked part time, LL worked overtime, often at nights (when babies are more likely to collapse). The neonatal unit Lucy worked on cared for poorly and premature babies requiring more intensive care.
- Professional statisticians have since performed statistical assessments that demonstrate a) there remains a systemic cause of infant still-birth and neonatal death at the COCH even when the so-called murder cases are removed from the data; and b) that the police table representing LL presence for all the events is a statistically normal artefact.
- A Royal Statistical Society (RSS) report, produced before the LL trial, laid out the standard methods from medical statistics and epidemiology which should be used to analyse such data in this and similar alleged serial killer nurse cases. It drew on the experience obtained from earlier cases, for example, that of Lucia De Berk, a nurse in a children’s hospital in the Netherlands, who was initially convicted because of a faulty statistical analysis. Lucia’s conviction was only overturned after analysis showed that the notion that her presence at so many deaths and other incidents could not be a coincidence had contaminated the medical judgements of medical experts called to give their opinion on individual events. Numerous recommendations of the RSS had already been grossly violated during the police investigation into the case of Lucy Letby by. the time the report was published. No statistical analysis of the roster data was performed at all.
2) Other possible causes of the neonatal deaths. The limited scope of the investigation.
No direct evidence implicating Lucy Letby was produced. No one saw her doing anything wrong. Instead, the jury was told that she must be guilty because all other possible causes of unexpected collapse and death had been investigated and eliminated, and that LL was the only link between the 25 incidents. This is untrue. There never was a wider, independent investigation by outside experts with the relevant scientific expertise. Indeed, a 2017 report by the Royal College of Paediatrics and Child Health (RCPCH) into the unit at the CoCH criticised the lack of systems in place in the hospital for reviewing such serious incidents. The report identified a series of problems in the unit, where the number and acuity of patients had expanded faster than resources available to look after them. These included significant understaffing, with gaps in doctor and nursing rotas, poor decision-making and insufficient senior consultant cover provided by paediatricians (the unit had no neonatologist), and lack of coordination to transfer very sick babies to the nearest Neonatal Intensive Care Unit (NICU). It recommended a wider independent expert and forensic investigation to look at possible medical causes of the unexplained deaths and collapses and the rashes some of the infants exhibited. Instead of this happening, the police were called in to conduct a criminal investigation which focused narrowly on looking for evidence that LL was a possible mass murderer. The main investigator and prosecution expert witness, Dr Dewi Evans, is a decade-long retired paediatrician, (not a forensic scientist or neonatologist specialising in intensive care neonates) who volunteered his services, and who has neither the expertise nor experience to make the scientific claims he made. Far from eliminating all other possible causes, alternative avenues of medical and scientific inquiry which could have pointed to different explanations for the deaths, were not followed up.
- At the time of their deaths, autopsies were performed for six of the babies. A natural cause of death was listed by a pathologist for 5 of them, and one cause of death was un-ascertained. These conclusions were overturned by the police investigation, even though there was no new evidence, with no explanation as to why.
- All but one of the children were born pre-term, several very pre-term. This makes them extremely vulnerable to infection. All the babies in the case showed many signs of viral or bacterial infection and all were listed as having “suspected sepsis”. Some of the babies had rashes and discolouration that the doctors said they had never seen before. The prosecution presented this as evidence that the babies were deliberately injected with air, based on a single scientific paper from 1989 which was not applicable to the babies in the LL case (see below). Viral or bacterial infections (including antibiotic resistant bacterial infections) and sepsis, which can also cause rashes and skin discolouration, were not presented as possible explanations to the jury.
- The police investigation did not include independent infectious diseases experts, forensic neonatal pathologists or toxicologists; no independent, scientific forensic investigation took place. Most worrying, there was no systematic investigation into possible viral or bacterial infections, even though the pattern of collapses and deaths fits an outbreak of infection. A nearby hospital had experienced a similar cluster of deaths within a short period just prior to events at CoCH. It was determined not to be the result of criminal action, with the deaths deemed to be natural. It is well known by epidemiologists and statisticians that clusters of unexpected deaths do occur within hospital settings, often due to outbreaks of unidentified infections.
- At the time of the collapses and deaths of the infants, enterovirus and parechovirus had been reported in other hospitals. There is a history of outbreaks of these viruses in neonatal wards in hospitals around the world. They especially harm preterm infants who do not yet have a functioning immune system. It is reported that many parents of the infants were concerned that their ward had a virus (as was Lucy). To date we have seen no evidence to show the hospital did any viral testing and, if they did, what the results were.
- At the same time as the increase in deaths in the CoCH neonatal unit, there was also a spike in stillbirths (often infection related) in the adjacent maternity unit.
- Both the maternity unit and the Neonatal unit at COCH had repeated raw sewage spills, providing an obvious explanation as to how a pathogen like an enterovirus (which is highly contagious through faeces) could have spread in the hospital.
- All the babies in the case were presented to the jury as being stable, before an unexpected and unexplained sudden collapse. This was highly misleading. All of the babies had “suspected sepsis” in the notes, with clear signs of an undiagnosed infection. They required resuscitation, mechanical ventilation and intubation. This was a very sick group of babies.
- Evidence from less well-resourced settings shows that death would be a normal and common outcome for babies in this category. Many would be expected to die after a sudden deterioration. Low staffing levels, leading to poor monitoring and poor infection control, are globally the big killers of preterm babies. In developed world settings babies are only kept alive by expert intensive care, with high staff-to-patient ratios and a focus on infection prevention. In this context, the low staffing levels at CoCH and the sewerage leaks are highly significant. While the death rate at CoCH was slightly higher than normally expected in the UK, it was much lower than the global average.
- The neonatal unit at CoCH was a level 2 unit offering mid-level specialist care for babies with severe health issues and prematurity. The prosecution claimed that neonatal deaths decreased after Lucy was taken off the unit. But in fact, the hospital, at the same time, downgraded the unit to level 1 (no longer taking in such sick babies), increased senior consultant cover and repaired the sewage spillage from the drains. This easily explains the decrease in neonatal deaths.
3) The insulin evidence.
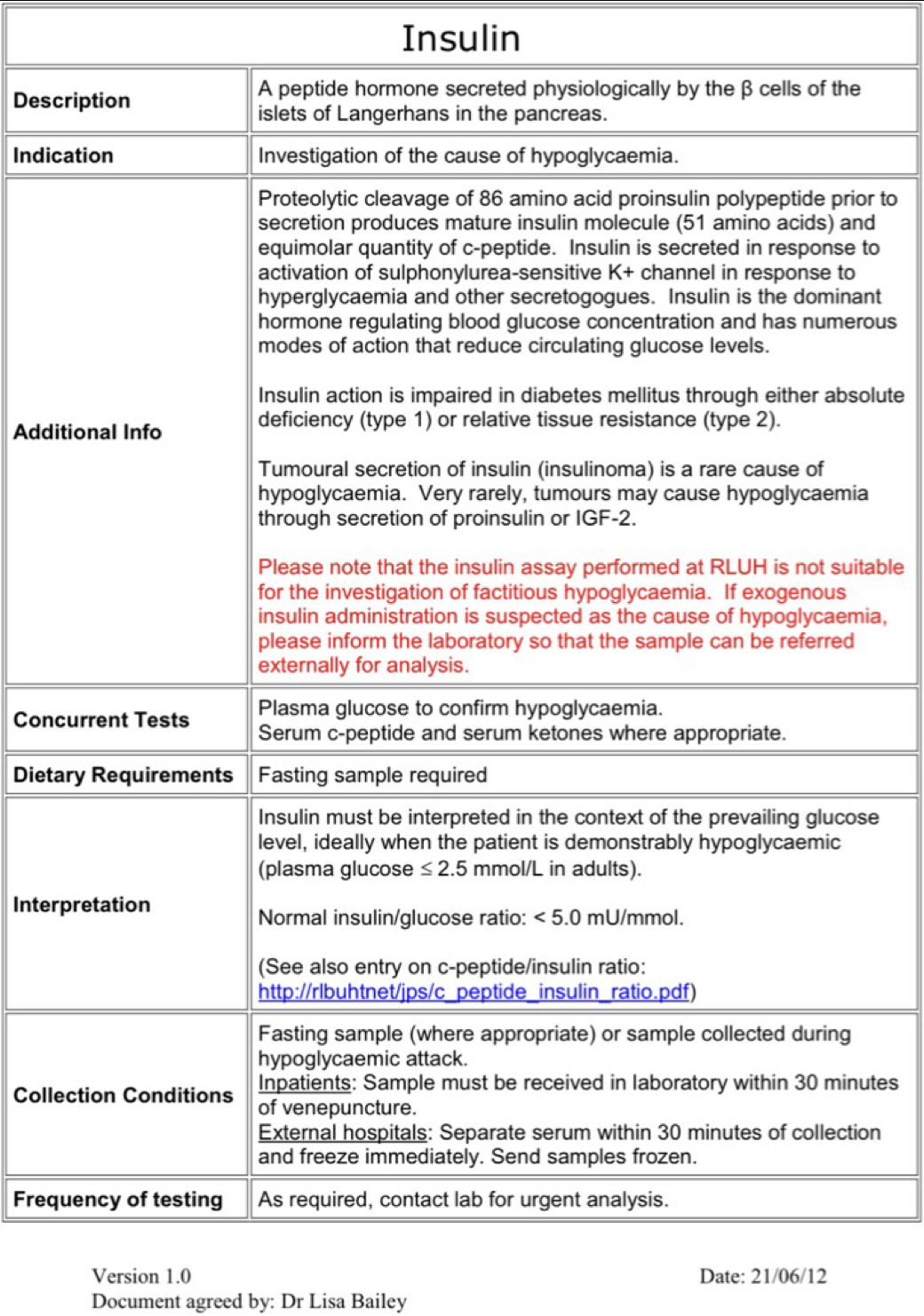
Soon into the police investigation, doctors discovered an entry in the notes of two babies who had died two years earlier, showing high levels of insulin and low levels of C-peptide. This was later presented to the jury and wider public as the key breakthrough which proved there was someone committing deliberate harm in the unit. Cheshire Police, in media reports like the Panorama programme, said this was the point that they focused all their efforts into a murder investigation. LL was accused of injecting insulin into the feeding bags of the two babies. These two hormones both derive from proinsulin, produced by the pancreas, leading to an expectation of related levels unless insulin has been injected, (although C-peptide levels can be higher as it has a slower clearance rate). Expert witnesses testified that deliberate poisoning with insulin was the only possible explanation. The defence accepted this as “established fact”, based on the testimony of the prosecution’s expert witnesses. This meant no defence expert witness was called to rebut this claim. However, the weight of expert opinion consulted since the trial is that there are better, innocent explanations for the two test results recorded in the notes, which were not presented to the jury. Guidelines for levels of evidence required in insulin poisoning cases were ignored. Other experts in the field say that two isolated tests with no possibility of follow-up or confirmation, were wholly inadequate for a murder conviction. (See also the section “opinions of other scientists re insulin” at the end of this post).
- The immunoassay lab tests used to establish the insulin and C-Peptide levels, are complicated and can give false results for many different reasons, one being the false-negative hook effect. One of the tests had such a high insulin level (4657 pmol/L), that lab specialists say this would almost certainly lead to a false negative for C-peptide, and so explain the discrepancy in recorded results. For an Insulin level of 4656 pmol/L, the predicted C-peptide concentration would be 99,277 pmol/L, which exceeds the parameters of the test. There is a hook effect at C-peptide concentrations that exceed 60,000 pmol/L. (The manufacturer of the blood test kit is “Coba”.)
- The Insulin assay test used is not designed to discover or measure the presence of injected insulin. Indeed, the lab where the tests were carried out states clearly on its website that its insulin assay tests are not designed “to measure exogenous insulin”, which would require a more precise (mass-spectrometry) test at an entirely different lab (Guildford RSCH Peptide Laboratory). This mass-spectrometry test was not carried out.
- Instructions from the forensic science regulator about the use of measurements like this in criminal prosecution were ignored. These state that there “must” be repeat samples, including a baseline blood sample taken before treatment starts; and further testing should have been required in order to confirm the values at a specialist laboratory. There must be reporting of possible sources of error and the likely sizes of errors, as well as a reporting of alternative explanations of anomalous outcomes. This was not done, so the tests should not have been accepted as forensic evidence. In many countries these assay tests are not accepted as forensic data for criminal prosecution because of all the possible errors from the collection of samples to procedures in the lab.
- The sample for baby F was not collected at the right time to diagnose exogenous insulin. This should have been done at the first episode of hypoglycaemia, prior to treatment. The blood sample was taken after multiple dextrose treatments; the insulin levels AFTER dextrose (glucose) were significantly raised. Multiple attempts to rectify the blood sugar would have increased the plasma insulin and suppressed the C-peptide. The babies should have been fasting three hours prior to the blood tests, which did not happen in this case.
- In neonates, there are a number of possible natural explanations for an unusual ratio of insulin to C-peptide, for example, autoimmune insulin syndrome (AIS), which were not presented to the jury. This is a highly specialist area requiring outside expert opinion, which was not sought during the investigation.
- A mother of one of the two babies was reported to have diabetes; therefore, the baby is more likely to have higher and less stable production of insulin as well as periods of low blood sugar (hypoglycaemia) shortly after birth, and during the first few days of life. (33.7% of all preterm neonates experience hypoglycaemia during this period – Sharma et al 2017). Likewise, clearance rates of insulin and C-peptide can vary much more in preterm babies than in children or adults, as organs like the liver may not be yet working properly.
- The link to Lucy Letby was conjecture. She was never seen injecting a baby, there is no direct evidence. The test for baby F was taken some 10 hours after LL’s shift ended, and after the TPN (intravenous feeding) bag had been changed. Baby L continued to have hypoglycaemia for a further 24 hours after LL left the ward.
- Expert witnesses testified that LL only needed to have injected a small amount of insulin into the TPN bag to reach the levels reported in the tests. These calculations have been challenged by other experts as they appear to be based on calculations for muscular rather than intravenous insulin injection. Intravenous fusion would require much higher doses of insulin.
- Both babies survived. Baby F tested a very high blood insulin concentration of 4657 pmol/L, C-peptide was 169 pmol/L and a blood glucose reading of 1.3 mmol/L. Within two hours of the blood test the baby’s blood sugar level was ~4 mmol/L. Normal glucose levels range between 1.5 and 6 mmol/L – so these readings are not particularly out of the ordinary. They are, however very surprising if the high blood insulin level recorded was accurate and a result of deliberate injection. Indeed it would be very surprising for the babies to have survived such an attack.
4) The evidence of deliberate injection of air
After mistakenly believing they had proved through the insulin evidence that there was a killer on the loose, police and doctors then looked for explanations as to how LL could have killed the other babies. She was accused of injecting them with air. She was also accused of pulling out ventilation tubes. But no direct evidence was presented for either claim. Indeed, the investigation did not follow normal scientific methods and once again there are much better explanations for the evidence presented. Indeed the evidence for air injection, which was claimed as the main murder method, totally ignores a large body of contradictory evidence.
- No forensic pathologists were involved in this investigation. Instead, it was carried out years after the deaths by Dr Dewy Evans, who is not qualified in this very specialist area. He approached the investigation like a doctor looking for a possible diagnosis, not like a scientist or pathologist looking for firm evidence. The jury, however, were told by the judge that they could trust his opinion as firm evidence.
- Conventional methods for investigating air embolism were not followed. These require specific post-mortem techniques, which were not carried out. Instead, two x-rays, taken more than 30 minutes after death and showing air in major blood vessels, were presented as evidence.
- One 1989 scientific paper was cited by Dr Evans to back up his theory. This paper was totally inapplicable to the case as it related to babies on aggressive ventilation treatments used at the time. The paper explicitly says post-mortem x-rays taken more than 30 minutes after death must not be used to determine air embolism, but in this case both the x-rays were performed beyond this time limit. “In 75% of reported cases the radiographs were taken antemortem. Post-mortem radiographs need to be interpreted with caution as intravascular air may appear as early as 25 minutes after death.”, (page 2 of paper). Relevant scientific papers were not included or presented to the jury.
- There are many other explanations for air in the veins after death which were not presented to the jury. A 2015 study, for instance, showed the majority of new-borns who had been resuscitated with CPR and subsequently died, had air embolism (Halbertsma et al) which showed up in scans taken after death. The babies in the Lucy Letby case, almost all received CPR. Air in the great vessels is also a common side effect from having tubes inserted into the baby’s umbilical lines and from intravascular injections.
- Another possible explanation for the radiological appearance of gas is sepsis. Jurors were told that Prof Owen Arthurs, radiologist at London’s Great Ormond Street Hospital, had been instructed to review X-rays taken of Child A – when alive and after death – as well as other babies in the investigation. He concluded that a line of gas in front of the spine was an “unusual finding” in a post-mortem x-ray which would be unlikely in deaths by natural causes, and which could be explained by air having been administered. But, he said, it has also been seen in road traffic accidents and cases of sepsis infection.
5) The “Confession” Note
Police found a handwritten note in LL’s home stating “I am Evil […] I did this” – which was presented to the jury as evidence by the prosecution.
- There were a multitude of handwritten notes. This was not unusual, as nurses are encouraged to journal as a component of their training.
- In the notes, LL also writes, “I’ve done nothing wrong […] how has this happened? […] Please help […] I feel very alone and scared […] no hope”. The guilt she expressed was clearly stated as worry that she might not have been “good enough” in her role as a nurse to save the babies who died while in her care.
- On BBC’S Panorama, Professor Emeritus criminologist David Wilson explained that these notes were not a confession but that they were instead “the ramblings and outpourings of someone under extreme psychological pressure and stress”, due to the nature of the accusations against her. He suggested that she could have meant that, “it is alleged I am evil […] It is alleged I did this”, referring in her notes to the serious accusations made against her by the doctors and the police.
- David Wilson stated that, in his experience of criminal cases, it is very common to see these types of notes written by people who in fact transpired to be innocent.
- Neonatal nurse Lucia de Berk and Kathleen Folbigg both had similar handwritten notes shown to the jury by the prosecution. Both were convicted and sentenced to life imprisonment, but years later both were exonerated after new medical, scientific and statistical expert evidence revealed their wrongful convictions.
- The code LD in her notes means “Long Day”, text commonly used by nurses to record shift notes.
A detailed analysis of the main “post-it note” shown to the jury is posted below. It demonstrates clearly that the note does not contain a confession.
6) The prosecution ignored the rules governing the use of Scientific experts and there was a lack of expert defence witnesses
The scientific experts used in the case did not behave as scientific expert witnesses must behave, according to the rules of CPS criminal prosecution. They are supposed to be strictly neutral (despite who is paying them) and they are supposed to always give alternative explanations and to mention scientific (and statistical) uncertainties. They did not do this. And they also spoke about scientific matters in which they have limited expertise. This applies not only to Dr Dewy Evans. Prof Hindmarsh has no expertise in forensic science in neonates. He also clearly did not know the relevant scientific literature concerning insulin poisoning, a specialist area which would not be in the knowledge of most practicing doctors. The defence appear to have accepted at face value the neutrality and expertise of the prosecution’s scientific witnesses and for some reason did not seek their own experts to challenge central conclusions of the case. Much of the material above, plus more analysis, was presented to the defence team before the end of LL’s trial. There was also an attempt made to present it to the judge as a “friend of the court”. But both were unsuccessful because rules prevent the defence calling new expert witnesses after a trial has started. So the jury never had the benefit of this evidence. In particular, no defence experts testified regarding strong evidence of a differential diagnosis of infection in every case and what that could mean. This left all the prosecution’s expert witnesses essentially unchallenged. While this could be dismissed by putting the blame on the defence team, this misses the point. In a case which relies on highly specialised medical and scientific evidence, it is perhaps unreasonable to expect solicitors, barristers, judges and other legal professionals to be able to evaluate the quality of evidence and find the right experts. Defence barristers also complain that it is often very difficult to find expert defence witnesses willing to testify in cases involving children. This points to much deeper systemic deficiencies related to the use of complex scientific and medical evidence in criminal cases. The same is true for the police and prosecution investigation. The very obvious and alarming errors in the investigation are not necessarily the result of a deliberate cover-up or bad intent. Rather they result from the lack of understanding of scientific processes and investigation and a lack of understanding of how to judge and grade the reliability of medical evidence. There is a more detailed discussion of these aspects below.
The wider implications of the Lucy Letby case for the use of science in criminal trials and the need for reform.
Scientific evidence today plays an increasingly important role in obtaining convictions in the criminal justice system. However, the use of deeply flawed science in the Lucy Letby case raises worrying questions as to how scientific evidence is assessed and presented to juries, and whether the whole system needs modernisation and reform if miscarriages of justice are to be avoided.
Normally scientific evidence is peer reviewed by a panel of suitable and carefully identified experts, before it is published. This is a vital step, not only to iron out mistakes, but also to ensure correct scientific methods are followed and that the evidence published is robust enough to justify any conclusions that are reached. Peer review is used because scientists are the only ones with sufficient knowledge and expertise to evaluate the work of their peers.
In terms of medical evidence there is then a further process of independent grading before producing guidelines for doctors and other medical practitioners to follow. Grading provides a guide for doctors, who are often not experts in scientific methodology or statistics, so they can evaluate how reliable evidence is. The process usually starts with a systematic review of all the literature about the topic. If the review does not show up relevant studies or clinical trials from which to draw firm conclusions, a panel of experts will make recommendations for medical practice based on their experiencer. This expert opinion is considered low quality evidence, and any recommendations will be heavily qualified, because panels of top medics are rarely unanimous in their opinions and are often shown to be wrong when more rigorous scientific studies are carried out.
Relevant observational studies, where researchers simply observe and record the impact of potential treatments in a systematic way, get a higher grade. The gold standard for evidence are Randomised Controlled Trials (RCTs), which are carefully designed experiments used to prove or disprove a particular theory. These have built in methods to remove the inevitable bias of the researchers, as well as the doctors and other medical staff actually involved in treating patients in the study, and to work out detailed estimates of potential benefit and harm. To get the highest grade of evidence, RCTs need to be big enough so that the results are statistically significant and could not be the result of chance. And their results need to be replicable and relevant to the wider target group of patients. Often medical practitioners will not accept a single RCT as a basis upon which to change practice, in case there were errors in the way it was conducted. There are sometimes prolonged debates with serious differences of opinion among expert opinion before new treatments are adopted, because even the conclusions of RCTs can turn out to be wrong.
In the legal system, too often none of this happens when scientific or medical evidence is presented to juries who are likely to have much less understanding of the scientific process than doctors. Investigations are often police led and may not follow a scientific process. The trial then relies on both prosecution and defence to find their own expert witnesses, in a process where there are few criteria set down for vetting the suitability of experts beyond how well they will come across to a jury. The judge and jury, who are bound to be out of their depth in terms of scientific knowledge, are left to assess the relative strength of evidence when witnesses disagree with each other, with little chance to pose questions. Within this adversarial courtroom process, it is extremely difficult for non-scientists, to evaluate where the weight of scientific opinion might lie, or the reliability of the evidence presented. In the Lucy Letby case, the jury and the legal professionals involved were clearly not equipped to understand the reliability (or lack or it) of the evidence presented in the prosecution case.
Because of the adversarial nature of the process, it is also very difficult for legal teams to find scientists willing to act as expert defence witnesses. Academics are worried about a public process where hostile lawyers may try their best to discredit them – not necessarily focusing on the quality of evidence or the science. And the process provides no mechanisms for experts watching from outside, to input their knowledge when they see mistakes being made. Indeed, once a trial has started new expert evidence or expert witnesses cannot be introduced.
The Lucy Letby case demonstrates clearly many of the most serious weaknesses of the criminal justice system with regard to scientific evidence. After a series of unexplained deaths in a public hospital, there should have been a broad independent science-led investigation to evaluate how serious a spike this represented and probable causes. Instead, after the police were called in, the investigation tunnelled into a criminal investigation focusing only on gathering enough evidence to prosecute Lucy Letby. Doctors working on the ward became the principal advisors to the investigation and then “expert” witnesses in the trial.
The prosecution investigation, led by a retired paediatrician, should never have been presented to the jury as reliable scientific evidence. Doctors and scientists have very different methods for carrying out an investigation. A doctor will come up with a differential diagnosis, listing all the possible causes of a patient’s symptoms. They will then work through the list, eliminating all the possibilities, often by trying different treatments, until they reach a diagnosis. Often this turns out to be wrong, which does not matter as long as the doctor keeps an open mind, is prepared to consult with colleagues who make have more specialist knowledge, and to change course in the face of new evidence. This not a scientific method. Medicine is often as much an art as a science and has to confront many aspects of disease where we are still fundamentally ignorant. This is especially true when working with neonates, who cannot talk or indicate what hurts and what their symptoms are.
The Lucy Letby investigation was led by doctors and carried out using this method. Dr Dewy talked about his “diagnosis” that the babies were killed by air embolism. It was a diagnosis reached after the event, without ever being able to examine the babies. It may have been his honest opinion, but it was not scientific at all and should never have been presented to the jury without very strong caveats and warnings about its inevitable limitations.
Defence lawyers, the judge and the jury cannot be expected to understand complex scientific and medical evidence – and the processes by which it needs to be gathered in order to be reliable. This is why in the LL case they accepted as scientific fact what was actually medical opinion, most of which would never have got through a scientific peer review. The defence team accepted that the insulin tests showed there was deliberate poisoning as “established fact”. The judge allowed evidence into the court that was not based on properly conducted forensic methods and told the jury they could trust an expert witness, who was a retired paediatrician and not qualified to make the statements he made. If it were graded, all of the evidence presented would have struggled to even be classified as “low quality” expert opinion, because no systematic review was carried out, and the expert witness was not qualified in the area where he gave testimony. It was a long, long way from proving guilt “beyond all reasonable doubt”.
And it was not only the legal professionals who were out of their depth. The journalists covering the case also had no idea of the correct questions that needed to be asked. Panorama produced a documentary which did not challenge the flawed scientific evidence relating to insulin and air embolism. While it would be easy to blame everyone involved for not doing their jobs – this misses the point. Rather the whole case shows the difficulties faced by non-scientists in evaluating complex medical and scientific evidence, if they are not trained to do so. It is the system which is at fault.
Neither is the case unique. There have been a series of other cases both in the UK and other countries where medical professionals have been convicted on evidence which would not have stood the scrutiny of a peer review process within the scientific community – leading to innocent people spending years in jail.
So is it time for a change? What kind of reform would be necessary?
The most basic tenets of our legal system lay down that a defendant is considered innocent until found guilty beyond all reasonable doubt by a jury of their peers. It is of fundamental public interest, not only that this happens, but that it is seen to happen. In terms of complex scientific evidence, perhaps the word “peer” needs to be extended to include a role for “peer review” and grading of scientific evidence before it is presented to a lay jury, to make sure that it is indeed up to standard to reach a threshold of “beyond all reasonable doubt”.
This would not require major changes in the way the criminal justice system works. It would also allow scientists to be consulted and input their expertise, without becoming part of such an adversarial courtroom drama, making it more likely that more scientists would agree to be involved. And it would mean that all this evaluation happens before the massive expense and potential damage of a criminal trial.
Without reform, there is a real danger not only of serious miscarriages of justice, but also that the criminal justice system is brought into disrepute, as some of the country’s leading scientific and academic minds start to question the basis for criminal convictions.
LINKS TO MORE DETAILED ARTICLES UPON WHICH THE SUMMARY IS BASED.
1) The Statistical Evidence.
Links to SoT articles: https://www.scienceontrial.com/post/shifting-the-data
Data obtained from FOI requests: https://www.whatdotheyknow.com/request/neonatal_deaths_and_fois#incoming-1255362
See especially, https://www.whatdotheyknow.com/request/521287/response/1255362/attach/html/3/FOI%204568.docx.html
2) Other possible causes of the neonatal deaths. The limited scope of the investigation.
Links to SoT articles: https://www.scienceontrial.com/post/a-malevolent-force
RCPCH Report: https://pdf4pro.com/cdn/www-coch-nhs-uk-7537c.pdf
NHS Sepsis symptoms: https://www.nhs.uk/conditions/sepsis/
Neonatal sepsis: https://www.ncbi.nlm.nih.gov/books/NBK531478/#:~:text=Signs%20and%20symptoms%20of%20neonatal,with%20poor%20perfusion%20and%20shock
Cluster of human parechovirus infections as the predominant cause of sepsis in neonates and infants, Leicester, United Kingdom, 8 May to 2 August 2016 https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2016.21.34.30326
3) The insulin evidence.
Links to SoT articles:
https://www.scienceontrial.com/post/criminal-justice-in-england-disagreeable-facts
https://www.scienceontrial.com/post/adhering-to-the-limitations-of-the-scientific-protocols
https://www.scienceontrial.com/post/the-insulin-c-peptide-ratio
Forensic Science Regulator: code of practice https://www.gov.uk/government/publications/statutory-code-of-practice-for-forensic-science-activities
Insulin assay test kit instructions: http://pathlabs.rlbuht.nhs.uk/insulin.pdf
A Nurse’s report of insulin: see attached file
C-peptide Suppression During Insulin Infusion in the extremely Preterm infant is associated with insulin sensitivity: https://pubmed.ncbi.nlm.nih.gov/31058966/
4) The evidence of deliberate injection of air
Links to SoT articles:
https://www.scienceontrial.com/post/endotracheal-tube-extubation-who-is-to-blame
https://www.scienceontrial.com/post/translating-the-science
1989 Air embolism paper, see (page 2) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1592039/pdf/archdisch00901-0075.pdf
Prevalence of systemic air-embolism after prolonged cardiopulmonary resuscitation in newborns: A pilot study, (Halbertsma et al, 2015) https://pubmed.ncbi.nlm.nih.gov/26092516/
Systemic Air embolism secondary to respiratory therapy in the neonate, (Marvin S Kogutt)
https://ajronline.org/doi/pdf/10.2214/ajr.131.3.425?download=true
Lucy Letby trial: Expert says ‘line of gas’ in post-mortem X-ray was ‘unusual’ but not diagnostic of air having been administered:
Normal perinatal and paediatric postmortem magnetic resonance imaging appearances:
https://link.springer.com/article/10.1007/s00247-014-3166-y
5) The “Confession” Note
https://www.scienceontrial.com/post/the-imagined-confession-examining-the-green-note
6) The lack of expert defence witnesses
This is a link to the complete evidence presented to the defence team before the end of the trial.
Opinions of other scientists and specialists which back up the insulin research:
- “Among all the tests performed by clinical labs, immunoassays have the highest inaccuracy. In addition to intrinsic inaccuracy being based on immunological interactions, numerous drugs and conditions could influence the data produced by immunoassays.” Adel Ismail, retired Head of Clinical Biochemistry and Director of Pathology Services, Pinderfiels and Leeds Teaching Hospitals, West Yorkshire. Area of speciality in laboratory medicine is in ensuring the diagnostic accuracy of measurements and interpretation of laboratory results.
- In his paper “Hypoglycaemia: accidents, violence and murder. Part 2, Prof V. Marks states, “Contrary to dogma, an inappropriately high plasma insulin and a low C-peptide concentration –especially in the presence of hypoglycaemia – though highly suggestive, is not pathognomonic of exogenous insulin administration,” Professor Vincent Marks, Emeritus Professor of biochemistry and leading authority on insulin in criminal law. In discussing the Letby case with Science on Trial, Prof Marks insisted that assay tests used in the Liverpool laboratory have no forensic value and should have been judged inadmissible by the court.
- In his paper “Forensic aspects of Insulin,” Prof V. Marks states, “A sample of venous blood must be collected, before any treatment is given, and separated into plasma or serum immediately, or as soon as practicable, and stored at -20 °C until analysed or discarded. At least one further blood sample should be collected, preferably about 1h after restoration of normoglycaemia, and stored alongside it.” In the case of both babies with hypoglycaemia, repeat insulin measurements were not taken.
- Marks (2005): “Cases that come to court and depend exclusively on the results of a single insulin assay should always be suspect as the methods of measurement employed generally do not meet forensic standards and/or their interpretation is questionable”.
- Vincent Marks claims a fatal dose of insulin for an adult human being is around 1000 units.
- Alan Wayne Jones (2023) says: “Analytical methods utilizing immunoassay, such as RIA, EMIT and ELISA, are mainly intended as presumptive, diagnostic, or screening tests for presence of drugs. In forensic toxicology, positive immunoassay results need to be verified by re-analysis with a more specific confirmatory method, such as GC-NPD, GC- MS or LC-MS/MS”.
- Alan Wayne Jones (2023) has almost the same statement as Vincent Marks: Practical Diabetes Int 2005; 22(9): 352–358, “Hypoglycaemia: accidents, violence and murder. Part 2”
Links to scientists’ research papers:
Insulin analogues as a new example of interference in insulin assays
https://journals.sagepub.com/doi/full/10.1177/0004563215590165
Adult hypoglycaemia; a narrative review on forensic aspects https://jlpm.amegroups.org/article/view/5995/html
Hypoglycaemia: accidents, violence and murder. Part 1 https://onlinelibrary.wiley.com/doi/epdf/10.1002/pdi.854
Hypoglycaemia: accidents, violence and murder. Part 2 https://onlinelibrary.wiley.com/doi/full/10.1002/pdi.875
A W Jones (2023): Insulin murder and the case of Colin Norris. https://www.sciencedirect.com/science/article/abs/pii/S1752928X2300001X
Forensic aspects of Insulin https://www.sciencedirect.com/science/article/abs/pii/S0168822713001861
Scientific working group for forensic toxicology, (SWGTOX) standard practices for method validation in forensic toxicology. J Anal Toxicol (2013), 37, 452 -447. https://academic.oup.com/jat/article/37/7/452/765476
Links to other articles and blogs/books:
In 2020, Doctors at The Countess of Chester Hospital missed chances to save Olly Thornton who died from sepsis after they discharged him from hospital. He received inadequate care; they didn’t screen him for a bacterial infection he had which led to sepsis. He exhibited the same rash on his body as did the babies Lucy is accused of killing. https://www.bbc.co.uk/news/uk-england-merseyside-67940167
Professor Richard Gill’s blog: https://gill1109.com/2023/05/24/the-lucy-letby-case/
Unlucky Numbers: Richard Gill is fighting the shoddy statistics that put nurses in prison for serial murder. Science, Vol 379, Issue 6629, 2022. https://www.science.org/content/article/unlucky-numbers-fighting-murder-convictions-rest-shoddy-stats
Dr David Robert Grimes, scientist and author: https://www.scientificamerican.com/article/bad-science-and-bad-statistics-in-the-courtroom-convict-innocent-people/
Two thirds of maternity units are dangerously substandard: https://www.theguardian.com/society/2023/oct/20/two-thirds-of-englands-maternity-units-dangerously-substandard-says-cqc
Matthew Syed, British journalist and author of “black box thinking” book. From a review: “In Black Box Thinking, Matthew Syed argues that learning from failure drives human progress. Namely, our politics, courts, and hospitals stigmatise failure and perpetuate a culture of false exceptionalism that prevents them from improving. If we neglect to improve our stagnating institutions, they’ll continue to take the lives of innocents—whether it’s death due to preventable medical error or wrongful conviction that leads to life in prison. ” https://www.matthewsyed.co.uk/book/black-box-thinking-the-surprising-truth-about-success/
Peter Elston, statistician, “Chimpinvestor” blog: https://www.chimpinvestor.com/post/do-statistics-prove-accused-nurse-lucy-letby-innocent
Scott McLachlan’s Law Health and Tech blog: LL Part 0: Scepticism in Action: Reflections on evidence presented in the Lucy Letby trial. https://lawhealthandtech.substack.com/p/scepticism-in-action
Anonymous nurse “report”: please see attached file
Lawrence George report of baby F and baby L : please see attached file.
The state of forensic science in the UK. “The UK’s forensic science used to be considered the gold standard, but no longer. The risk of miscarriages of justice is growing. And now a new Westminster Commission is trying to find out what went wrong. Joshua talks to its co-chair, leading forensic scientist Dr Angela Gallop CBE, and to criminal defence barrister Katy Thorne KC.” https://www.bbc.co.uk/sounds/play/m001k7vt
Toxic doctors put patients at risk, says NHS Watchdog. From sepsis to maternity, the ombudsman says he is shocked by failings every day, https://archive.li/ItXoi
Announcement follows campaign by parents of Martha Mills, 13, who died in hospital after developing sepsis https://www.theguardian.com/society/2023/sep/14/government-backs-marthas-rule-on-second-medical-opinion-in-england
Bad stats overturn medical murders podcast https://www.science.org/content/podcast/bad-stats-overturn-medical-murders-and-linking-allergies-climate-change